When fatty deposits accumulate along the inner walls of coronary arteries over years, they transform into hardened plaque that restricts blood flow to the heart muscle. This progressive narrowing of arteries, medically termed atherosclerosis, represents one of the most serious threats to cardiovascular health, potentially triggering heart attacks, stroke, or sudden heart failure. Managing this condition traditionally requires a multifaceted approach combining lifestyle modifications with pharmaceutical interventions and, in many cases, surgical procedures to restore normal circulation. However, when plaque becomes severely calcified—essentially turning into bone-like deposits—conventional treatment strategies often reach their limits, presenting cardiologists with a uniquely challenging clinical problem that demands innovation.
Plaque accumulation within arteries involves a complex mixture of lipids, cholesterol, calcium deposits, cellular debris, and fibrin, a protein that promotes blood clotting. Over time, this heterogeneous material builds up layer by layer, progressively narrowing the vessel lumen until blood flow becomes critically restricted. The consequences can be catastrophic. Narrowed vessels force the heart to work harder while delivering less oxygen-rich blood to vital organs. The situation deteriorates further when plaque ruptures or when clots form on the damaged surface, potentially blocking vessels entirely and causing acute myocardial infarction or cerebrovascular events. Understanding the composition and mechanisms driving plaque formation has been crucial to developing effective interventions.
Conventional interventional cardiology techniques—including percutaneous coronary intervention, coronary artery bypass grafting, and standard balloon angioplasty—work reasonably well for soft or moderately calcified plaques. In these cases, cardiologists can insert a balloon catheter that, when inflated, compresses the plaque material against the vessel wall, widening the lumen. They then deploy a metal stent, a small expandable scaffold that maintains the widened passage and prevents the artery from narrowing again. However, this straightforward approach becomes significantly more difficult when calcium deposits dominate the blockage, creating what consultant cardiologist Datuk Dr Tamil Selvan Muthusamy describes as essentially trying to crack open a stone. Severely calcified lesions resist balloon expansion, frequently resulting in incomplete revascularization and poor long-term patient outcomes.
When traditional methods prove inadequate, specialists turn to specialized techniques including rotational atherectomy, high-pressure balloon inflation, and intravascular lithotripsy to address calcium burden. Intravascular lithotripsy, or IVL, represented a genuine breakthrough when it emerged, using focused ultrasound energy delivered through a specialized catheter to generate acoustic waves that fracture calcified plaque. The principle is elegant: carefully controlled sound energy can shatter hardened calcium without harming surrounding healthy tissue. Yet despite its innovation, standard IVL systems have significant practical limitations that have constrained their effectiveness in clinical practice.
The conventional IVL technology relies on an external energy generator that produces ultrasound pulses transmitted through the catheter to the blockage site. As Dr Tamil Selvan explains, physicians face strict constraints on the number of pulses available—older systems provided only eight pulses to fracture calcium throughout an entire lesion, though newer versions offer twelve. This rationing means clinicians must strategically decide where to deploy limited acoustic energy, potentially leaving some calcification untreated. Additionally, the standard IVL catheter design is relatively bulky, making insertion into small coronary arteries technically challenging, particularly when the vessel lumen is already severely narrowed by disease. This limitation frequently necessitates additional complex techniques and prolongs procedures.
Another fundamental problem with existing IVL systems relates to anatomical variability. Coronary arteries are not uniform tubes; they taper gradually, beginning perhaps at 3.5 to 4 millimetres in diameter before narrowing to 2 to 3 millimetres as they branch and extend distally. Current IVL balloons come in fixed sizes—a 3-millimetre balloon must fit vessels ranging from 3 millimetres to 2 millimetres, making optimal contact difficult. Poor contact between the device and vessel wall reduces efficacy and increases the risk of complications. For lengthy blockages spanning multiple vessel segments of varying diameters, physicians must exchange devices repeatedly, adding time, cost, and procedural risk. These technical constraints have meant that some patients with extensive calcified coronary disease remain inadequately treated despite available interventions.
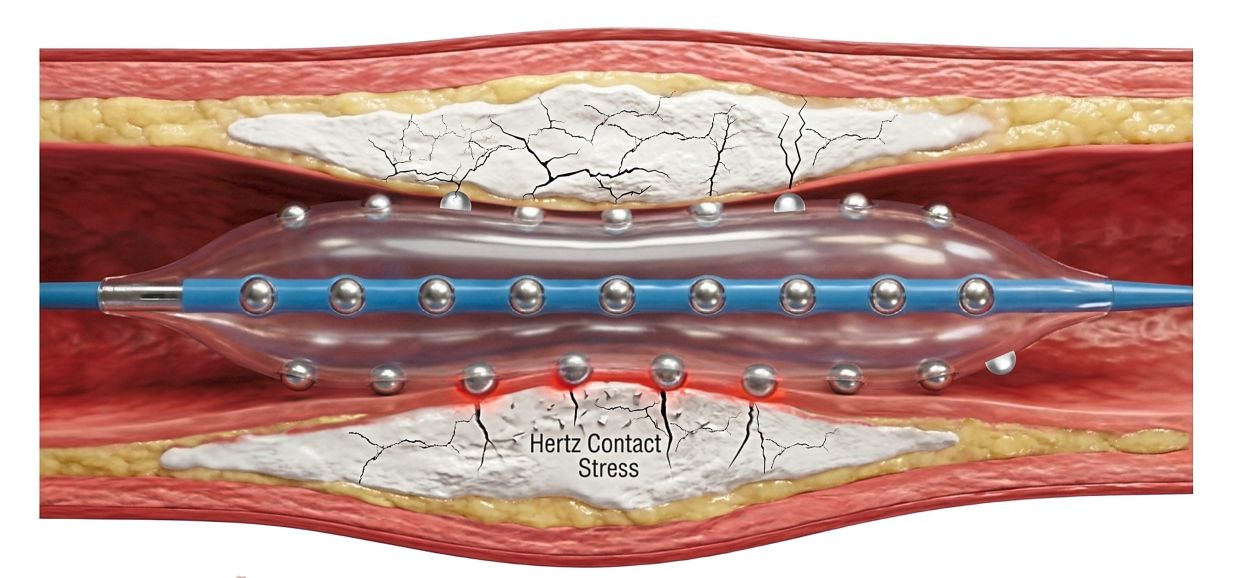
Recognizing these limitations, Malaysian cardiologists identified an opportunity to evaluate an innovative solution. During 2025, Dr Tamil Selvan's research team embarked on a clinical investigation of the Hertz Contact-IVL System, a fundamentally redesigned lithotripsy platform that abandons the external energy approach in favour of integrated mechanical design. Rather than relying on acoustic waves generated outside the body, the HC-IVL system employs a balloon embedded with precisely positioned metallic hemispheres, typically made from stainless steel. When the balloon inflates against a hardened plaque surface, pressure applied to these hemispheres becomes mechanically amplified and transmitted with concentrated force directly to the calcium deposit, creating deep fractures that split the hardened material apart.
This mechanical approach offers multiple practical advantages over energy-based lithotripsy systems. First, it eliminates the external energy constraint; physicians need not ration pulse applications because the mechanical fracturing process operates differently, allowing treatment of longer lesions or larger calcium burdens with a single device. Second, the improved design dramatically enhances deliverability—the catheter navigates through severely narrowed vessels more readily, reducing the need for additional techniques or device exchanges. As Dr Tamil Selvan emphasises, a single HC-IVL balloon can often treat extensive disease throughout an entire coronary artery tree, substantially simplifying the procedure from both technical and logistical perspectives. Third, the mechanical fracturing mechanism creates deep, wide cracks in the calcium without damaging surrounding arterial tissue, allowing subsequent stent expansion to be more complete and reliable.
The HC-IVL system operates without relying on an external ultrasound generator; instead, it transmits mechanical pressure through the integrated hemispheres, creating what cardiologists term a mechanical lithotripsy approach. When the stainless steel hemispheres contact the hard calcium surface, applied balloon pressure multiplies across these contact points, concentrating tremendous force in micro-regions where the calcium lies. This focused pressure amplification exceeds what simple balloon inflation alone could achieve, effectively shattering even severely hardened deposits. The resulting fractures are deeper and more extensive than those produced by standard IVL, better preparing the lesion for stent placement and reducing the risk that the artery will renarrowing after the procedure.
Dr Tamil Selvan and his colleagues made a strategic decision to undertake comprehensive safety and efficacy evaluation at the Malaysian level. While the device developer had conducted initial research involving multiple smaller studies across several United States centres, the local research team recognised that a larger, well-designed investigation conducted in Malaysia was necessary to fully characterise performance and safety across diverse patient populations. This approach reflects the principle that device performance can vary based on patient demographics, disease characteristics, procedural practice patterns, and healthcare infrastructure—factors that may differ between American and Malaysian settings. By conducting robust local research, the team generates evidence specifically relevant to Southeast Asian cardiology practice.
The study's significance extends beyond mere technology evaluation. Coronary atherosclerosis with calcification represents a growing healthcare burden throughout Malaysia and the region as populations age and metabolic risk factors like diabetes and hypercholesterolaemia become increasingly prevalent. Current treatment options for severely calcified disease remain suboptimal, leaving some patients with limited revascularisation options or worse long-term outcomes. Successfully validating the HC-IVL system could provide Malaysian cardiologists with a substantially improved tool for managing these challenging cases, potentially improving clinical outcomes for thousands of regional patients facing advanced coronary disease. Moreover, Malaysian-led research contributing to the global evidence base for innovative cardiac devices positions the nation as a contributor to cardiovascular medicine advancement, potentially attracting further investment in cardiac research and innovation infrastructure.
The investigation conducted by Dr Tamil Selvan's team addresses a critical gap in current technology options for complex coronary interventions. By systematically evaluating the HC-IVL system's safety and efficacy in a larger patient cohort than previously studied, Malaysian researchers provide clinically relevant data that could reshape how cardiologists approach heavily calcified coronary disease. The research also highlights how regional medical teams can contribute meaningfully to global clinical evidence while generating locally applicable insights. Should the HC-IVL system demonstrate superior safety and efficacy profiles, it could become standard therapy for calcified coronary disease throughout Southeast Asia, fundamentally improving care for patients facing some of cardiology's most technically demanding diagnostic situations.

